|
By Avery Hinks Lifting heavy weights, in or outside of the gym, involves both a lifting and a lowering phase. The lifting phase is called a concentric contraction, with your muscle shortening to move the weight against gravity. To then put the weight back down, your muscles perform an eccentric contraction, now lengthening back to their starting position as you control the weight’s descent. Researchers have spent years understanding the distinct influences of these two types of muscle contractions on performance. In general, training focusing on concentric contractions makes a muscle wider to emphasize strength. Eccentric training, conversely, makes a muscle longer, ideally to improve its speed and range of motion. 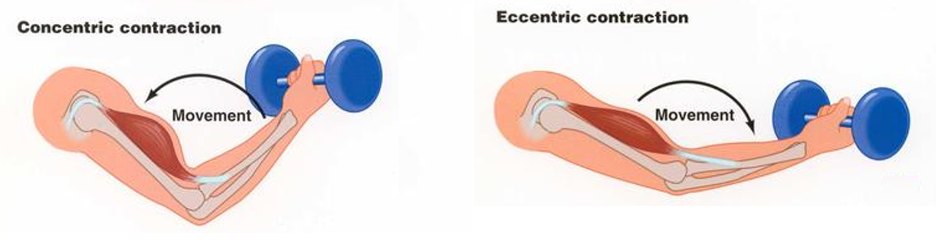 This all applies to what we call “skeletal muscles.” Those are muscles that connect one bone to another to allow your body to move. There is one muscle in the body, though, that contracts more than any muscle in your arms or legs, working constantly throughout your life, yet it does not connect bones together. I’m talking about the heart. The heart has no way of lifting or lowering weights, so the concentric vs. eccentric training paradigm described above wouldn’t apply to it, right? Actually, you can in fact train your heart both concentrically and eccentrically, and it’s less complicated than you might think (I see that image in your head of you trying, impossibly, to use your heart to lift a dumbbell). Allow me to explain… What does the heart do?The heart maintains the flow of blood to all the tissues of the body, including muscles, digestive organs, the skin, and the heart itself. Without blood flow, there would be no way for these tissues to receive the oxygen and nutrients they need, nor a way to have their waste products removed. These processes are necessary whether we are exercising or at rest. Sounds like it could be complicated, but thankfully blood flow is captured by a simple equation: Q = HR x SV In the equation above, HR represents heart rate, which is the number of times the heart beats in one minute. SV is stroke volume, which describes the volume of blood ejected by the heart on each beat. Putting these together, Q is our “cardiac output”: the volume of blood in litres pumped by the heart in one minute. In humans, normal cardiac output at rest is about 5 litres of blood per minute. To regulate the pumping of blood, the heart is divided into four chambers. On the top are the smaller right and left atria, and on the bottom are the larger right and left ventricles, as pictured below. 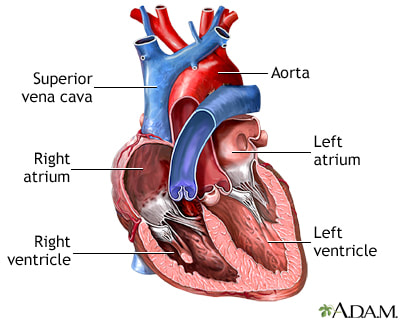 Blood enters the heart through the atria, then as the heart relaxes, that blood passes into the ventricles. The heart then contracts, and the ventricles pump blood to the lungs (right ventricle) to pick up oxygen, and to the rest of the body (left ventricle) to deliver oxygen. The heart contracts from the bottom up in a twisting motion, kind of like ringing water from a cloth. That twisting motion squeezes blood out of the ventricles and into circulation.  From the paragraph above, we can pick out two crucial factors that determine how much blood the heart can pump: contraction and relaxation. The heart’s ability to contract is important because a weaker contraction means less blood is ejected (in other words, stroke volume is lower). If the heart also has trouble relaxing, not enough blood will flow into the left ventricle from the left atrium in the first place. These limitations aren’t much different from how we view skeletal muscles. Weakness in the muscles of our arms and legs limit how much we can lift. If we also can’t relax those muscles, they become fatigued, more rigid, and overall less efficient. On a molecular level, heart and skeletal muscle are similarHeart muscle fibres and skeletal muscle fibres possess fundamentally the same molecular structure. Both are comprised of thousands of small units called sarcomeres. Each sarcomere contains the proteins actin, myosin, and titin, which generate force. Both heart and skeletal muscle fibres are also wrapped in structures called the sarcolemma and sarcoplasmic reticulum which together convert electrical signals into the chemical processes that incite muscle contraction. They also both contain mitochondria for the production of ATP for energy, and a nucleus to control gene expression. 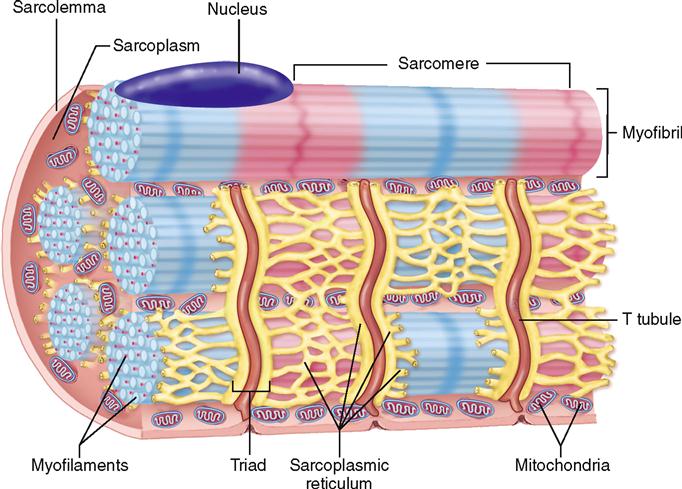 To perform its distinct actions, however, muscle fibres of the heart bear some differences to skeletal muscle fibres. Heart muscle fibres are shorter and more branched amongst each other, allowing them to better contract as a unit to eject blood. Adjacent heart muscle fibres are also connected by structures called intercalated discs. Intercalated discs transmit currents from one fibre to the next, further synchronizing the efforts of all fibres together. 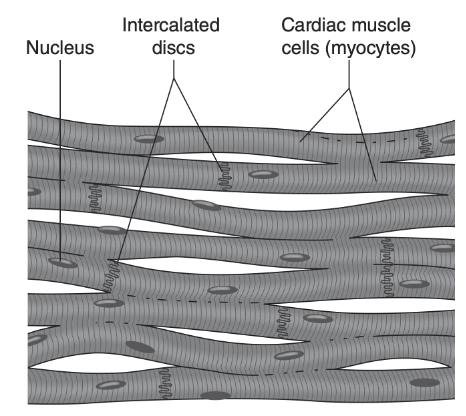 If heart muscle and skeletal muscle are so similar, does that mean we can train heart muscle like skeletal muscle? Concentric and eccentric training of heart muscleThe heart’s stroke volume is modified by both a preload and an afterload. Preload refers to the volume of blood that fills the left ventricle. Afterload is the pressure in the aorta that the left ventricle must push against when it contracts to eject blood. The distinct stimuli provided by preload and afterload are what distinguish between eccentric and concentric training of the heart. 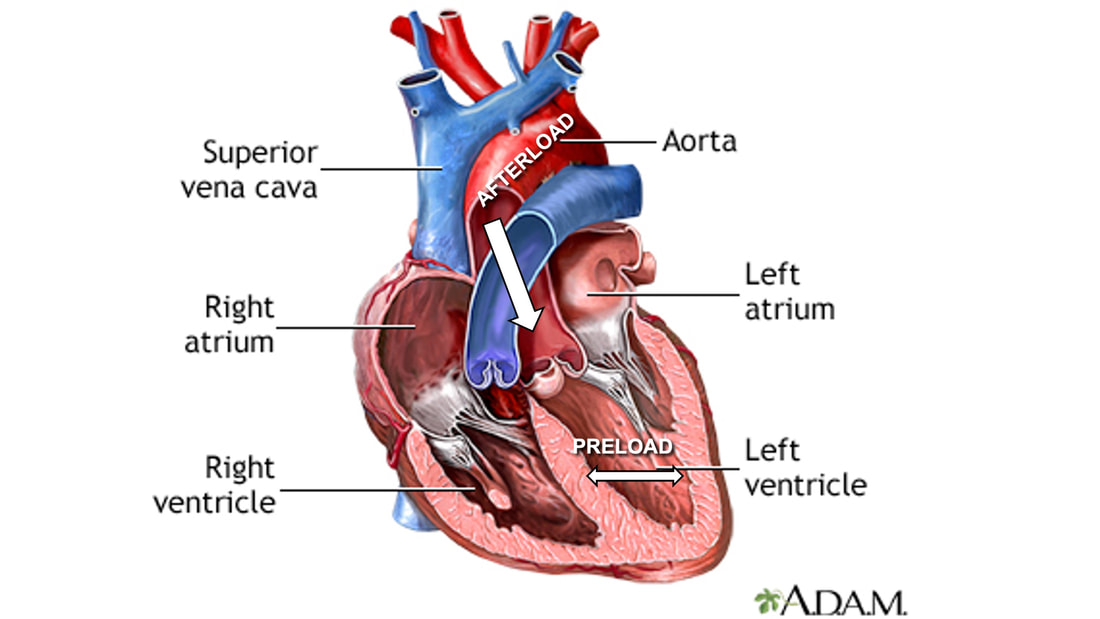 Endurance training includes any form of exercise with sustained movement for a long duration—exercises like jogging, cycling, or rowing. During these exercises, muscles go through cycles of contraction to create what’s called a muscle pump. When muscles contract, they compress the veins around them, pumping blood back the heart. Many continuous cycles of this muscle pumping action increases the overall amount of blood that returns to the heart. In other words, it increases the preload. The left ventricle stretches to accommodate this increased preload, creating a volume stimulus not unlike an eccentric contraction stimulus for skeletal muscles. If endurance exercise is repeated consistently over time, the heart remodels accordingly. 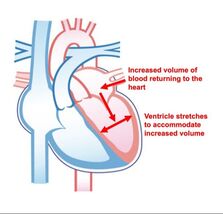 “Eccentric hypertrophy” of the heart is marked by an increase in the cavity size of the left ventricle. This increased cavity size accommodates the increased filling during endurance exercise. At the same time, there is also a proportional increase in the thickness of the muscle surrounding the left ventricle to ensure the left ventricle’s contractility is maintained with its larger size. Together, these adaptations amount to an increase in stroke volume. In other words, the heart becomes capable of ejecting more blood with each beat. 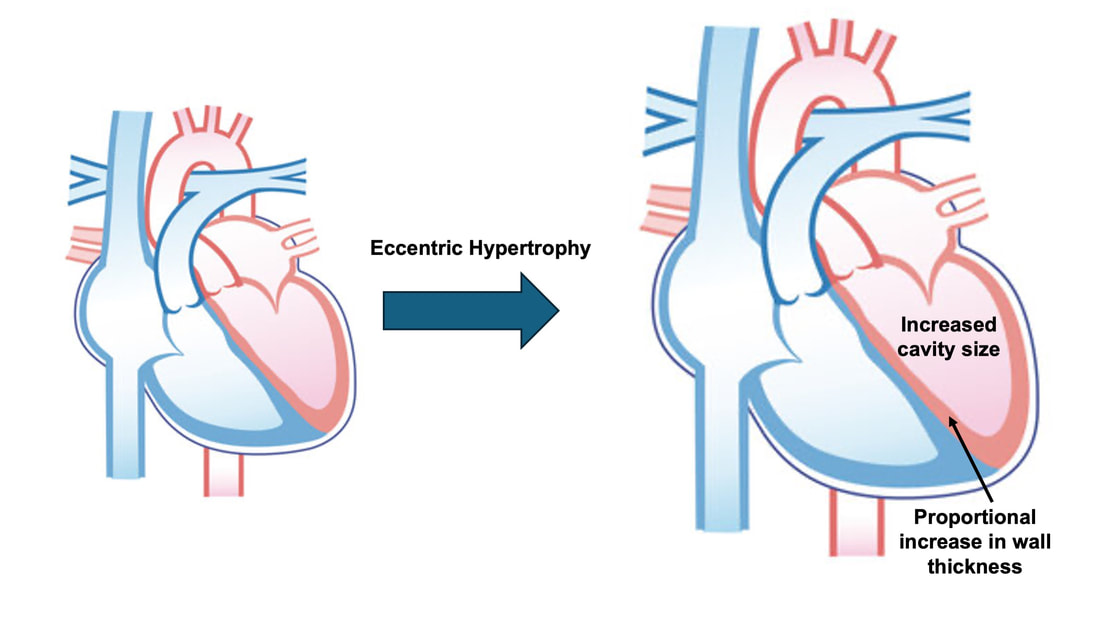 “Concentric hypertrophy” of the heart involves increasing afterload. This stimulus happens with resistance training—any form of exercise involving intermittent, high intensity muscle contractions that cannot be sustained for long. The most prominent example is weightlifting. When we lift heavy weights, we perform what’s called a “Valsalva maneuver.” Think of a time you lifted something heavy. Do you remember briefly holding your breath, clenching all the muscles of your torso, and breathing out forcefully as you performed the hardest part of the lift? That forceful exhale is the Valsalva maneuver. Valsalva is not necessarily bad, though—we do this as a natural tendency to stabilize our bodies to prevent injury. The Valsalva maneuver creates a large increase in pressure around the heart, which, of course, increases the afterload in the aorta. The left ventricle must then contract harder to pump blood out. If we repeat this type of exercise over time, we create a pressure stimulus on the heart similar to the concentric contraction stimulus we can give skeletal muscles. 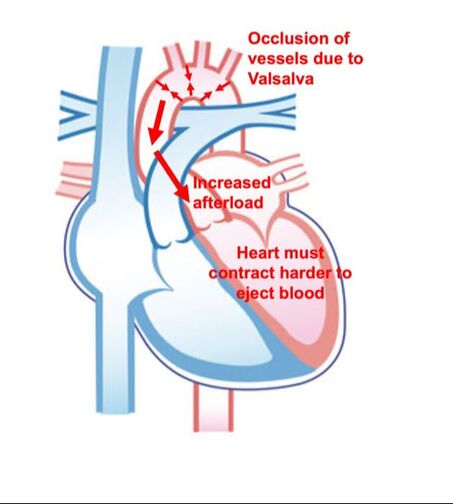 The heart adapts to the pressure stimulus by increasing the thickness of the muscular wall surrounding the left ventricle. With more muscle around the left ventricle, it gains a better ability to maintain stroke volume against a large afterload. Unlike endurance training, however, this increase in wall thickness with resistance training usually happens without a proportional increase in the left ventricle’s cavity size. Therefore, the heart’s ability to increase stroke volume with resistance training would be more due to an enhanced ability to contract the left ventricle than increased filling. 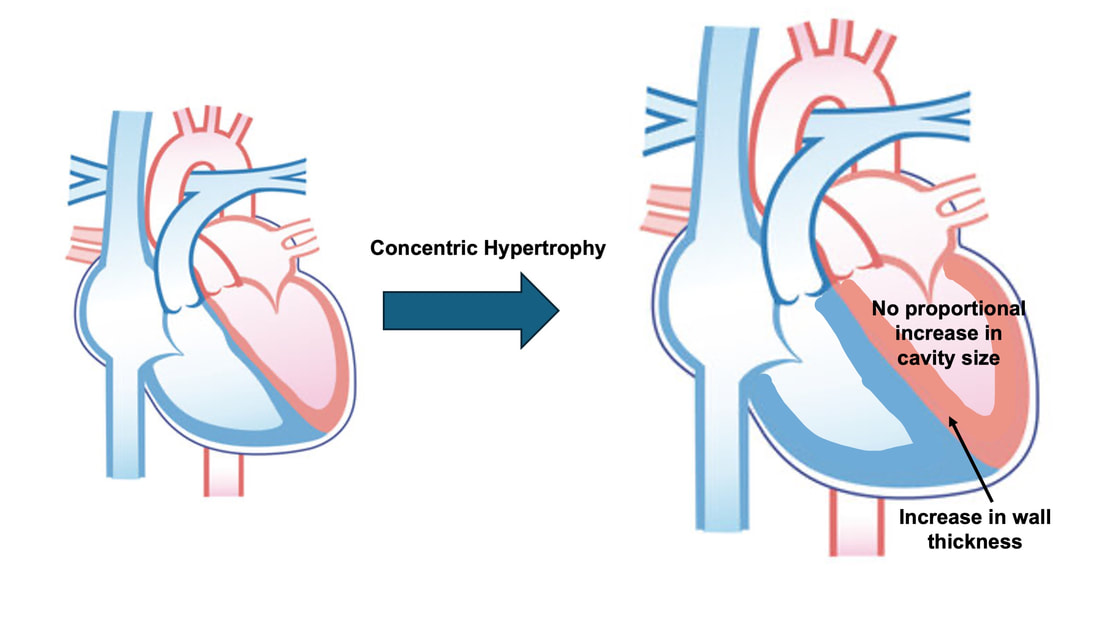 What is the functional significance?These divergent cardiac adaptations between endurance and resistance training could advantage or disadvantage the heart depending on the situation. A paper by Shave and colleagues in 2019 illustrated this paradigm nicely. They compared two groups of athletes: long distance runners and American football linemen. The runners exhibited heart dimensions consistent with eccentric hypertrophy while the linemen exhibited concentric hypertrophy. The researchers presented both groups of athletes with two challenges:
As a reminder, eccentric hypertrophy results from a volume stimulus on the heart, while concentric hypertrophy results from a pressure stimulus. With that in mind, it’s not surprising which challenge was handled better by which type of athlete. Faced with the infusion of saline, the heart would need to increase stroke volume to circulate the suddenly greater amount of blood. Both groups of athletes could do this, however, the long distance runners increased their stroke volume to a much greater extent. They could do this because their larger left ventricle cavity size is built to accommodate an increase in venous return during running. These findings are shown on the graph below, where the orange triangles on the top part of the graph represent runners (up to a 20% increase in stroke volume), whereas the purple triangles represent football linemen (up to a 10% increase in stroke volume). 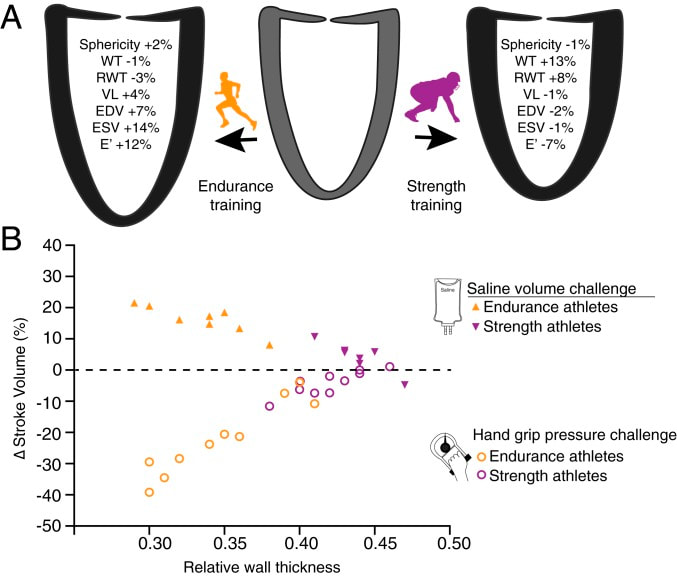 Conversely, the maximal handgrip exercise increases the afterload on the heart, which would work to decrease stroke volume. That is exactly what happened in the long distance runners, who experienced as much as a 40% drop in stroke volume, shown by the orange circles on the graph above. The purple circles, however, show that football linemen could maintain their resting stroke volume much better. Their greater wall thickness permitted them a better ability to increase contractility to overcome the elevated afterload. Eccentric or concentric remodelling of the heart…is one better than the other?The adaptations placed on the heart by endurance training and resistance training have different advantages for heart function. We could then ask the question: which adaptations are better for day-to-day life? Many would argue that eccentric hypertrophy of the heart is healthier, thus endurance training is better than resistance training. I would half agree with that. Eccentric hypertrophy is indeed healthier long-term. Concentric hypertrophy of the heart is not only observed with resistance training—it also observed with cardiovascular disease. Stiffer arteries and a higher blood pressure force the heart to contract harder to maintain a sufficient cardiac output. In this case, the resulting increase in wall thickness would be labeled “pathological concentric hypertrophy.” Multiple studies have pointed out that a higher blood pressure and arterial stiffness are sometimes observed alongside resistance training-induced concentric hypertrophy as well. The keyword above is sometimes. Resistance training could in fact produce whole-body cardiovascular adaptations that are similar to those seen with cardiovascular disease. However, that is usually only observed with high intensity resistance training. How “high intensity” am I talking about? A study by Miyachi and colleagues in 2004 subjected a group of men to whole-body resistance training at 80% of their maximum strength 3 days/week for 4 months. They observed a 30% increase in stiffness of the carotid artery following training. 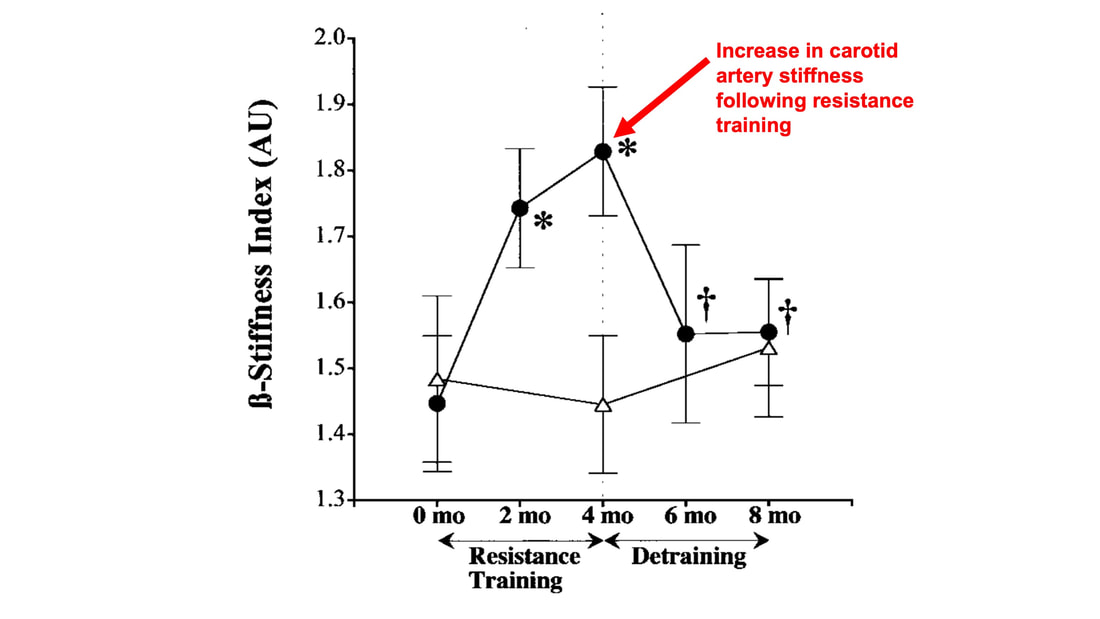 But of course they did with a training program like that! If you impose such high pressure loads on the cardiovascular system throughout the whole body so frequently, arteries will need to stiffen in order to protect themselves. Review papers by Haykowsky and colleagues (2002) and Pluim and colleagues (2000) compiled the results of multiple resistance training studies. They showed that low to moderate intensity (i.e., using weights less than 80% of maximum), balanced resistance training programs do not pose the kind of threat to the heart that the 2004 study above might frighten you with. In many cases, resistance training does not impair the heart’s diastolic function (ability to fill with blood) nor systolic function (ability to eject blood), which are both impaired alongside pathological concentric hypertrophy. Some studies have even reported remodelling of the heart closer to eccentric hypertrophy following low or moderate intensity resistance training.  The best recommendation I can give is one many have given before me: for the best results, do a bit of both. Get your resistance training in to strengthen your skeletal muscles, but maybe don’t do full-body, high-intensity resistance training 3 days/week. That alone might be enough for beneficial cardiac adaptations, but for good measure, and to better sway your heart toward eccentric hypertrophy, you should throw in some endurance training as well.
References Shave RE, Lieberman DE, Drane AL, Brown MG, Batterham AM, Worthington S, Atencia R, Feltrer Y, Neary J, Weiner RB, Wasfy MM, Baggish AL. Selection of endurance capabilities and the trade-off between pressure and volume in the evolution of the human heart. Proc Natl Acad Sci U S A. 2019 Oct 1;116(40):19905-19910. doi: 10.1073/pnas.1906902116. Epub 2019 Sep 16. PMID: 31527253; PMCID: PMC6778238. Miyachi M, Kawano H, Sugawara J, Takahashi K, Hayashi K, Yamazaki K, Tabata I, Tanaka H. Unfavorable effects of resistance training on central arterial compliance: a randomized intervention study. Circulation. 2004 Nov 2;110(18):2858-63. doi: 10.1161/01.CIR.0000146380.08401.99. Epub 2004 Oct 18. PMID: 15492301. Haykowsky MJ, Dressendorfer R, Taylor D, Mandic S, Humen D. Resistance training and cardiac hypertrophy: unravelling the training effect. Sports Med. 2002;32(13):837-49. doi: 10.2165/00007256-200232130-00003. PMID: 12392444. Pluim BM, Zwinderman AH, van der Laarse A, van der Wall EE. The athlete's heart. A meta-analysis of cardiac structure and function. Circulation. 2000 Jan 25;101(3):336-44. doi: 10.1161/01.cir.101.3.336. PMID: 10645932.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
AuthorAvery Hinks Archives
September 2023
Categories |
 RSS Feed
RSS Feed
